85
Fundus autofluorescence in age-related macular degeneration
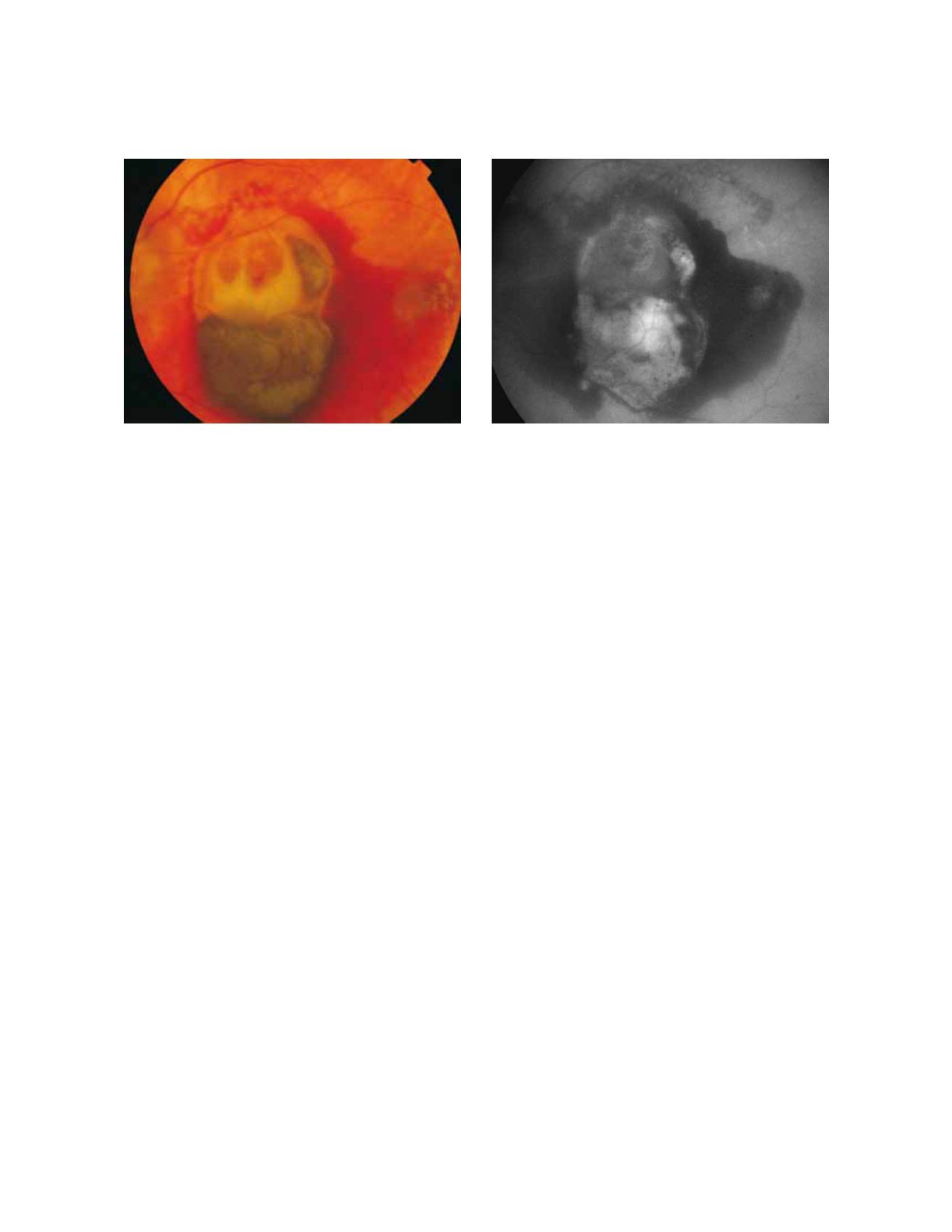
Figure 3 - Fresh haemorrhage in the left eye from a patient with choroidal neovascularization secondary to AMD. Fresh haemorrhages typically
appear dark due to blocked fluorescence. (A) Colour fundus and (B) fundus autofluorescence photographs.
A
B
be obtained from a quick and minimally invasive explora
tion with FAF. The decreased FAF intensity may also be
associated with hyperpigmented areas due to the mela
nin absorption of light
(35,39)
. However, it should be con
sidered that other fluorophores than LF can be found in
RPE and become more prominent in AMD patients, and
hyperpigmented areas may also cause an increase in the sig-
nal, which is supposed to result from the accumulation of
melanolipofuscin.
Other changes in FAF which are not related to RPE defects
may appear in AMD. Fresh haemorrhages typically appear
dark due to blocked fluorescence (Fig. 3). However, these
haemorrhagic areas eventually synthesize substances and
fluorophores, which are observed in the fundus as yellow-
ish areas and in FAF images as increased signals
(40)
(Fig. 4).
Pigment epithelial and neurosensory detachment and areas
with extracellular fluid accumulation associated with exuda-
tive lesions can be observed in FAF as increased or decreased
signal intensity.
Fluid accumulation under pigment epitheliumdetachment,
extracellular deposition of material under the RPE (drusen),
and fluid originated from CNV can occur with increased,
normal or decreased FAF intensity. This phenomenon is a
consequence of the presence of unknown autofluorescent
molecules other than LF, in the same spectral range than LF.
FAF imaging alone may not distinguish between melano-
lipofuscin from RPE cells migrated into the neurosensory
retina and LF within the normal RPE layer. It is always nec-
essary to compare the FAF findings with those from other
techniques such as fundus photograph, reflectance image,
fluorescein angiography or optical coherence tomography
(OCT)
(35, 39)
.
3.2.1 FAF in early AMD
Early AMD is characterised by the appearance of
localized RPE hypo or hyper pigmentation and drusen.
Drusen are formed by the accumulation of extracellu-
lar deposits in the inner aspects of Bruch’s membrane
(3)
.
Depending on their size and morphology, they can be
classified as hard or soft drusen. The molecular composi-
tion of drusen is quite complex and has not been com-
pletely elucidated (Fig. 5).
FAF changes in early AMD have already been reported
by several authors
(9,21,25,27,33-36,41)
; all of them concluding
that the changes in ophthalmoscopy and fluorescein
angiography are not necessarily related with FAF, suggest
ing that FAF may provide new information regarding the
stages and activity of the disease. Differentiation between
RPE LF and sub-RPE deposits with FAF images in vivo
can be a hard work.
An analysis of the variability of FAF in patients with
early AMD was recently reported by an international
workshop on FAF phenotype in early AMD. Among
their conclusions, a new classification system with eight
different FAF patterns was given
(39)
.
Normal pattern
characterized by a homogeneous
background autofluorescence with a gradual fluores-
cence decrease in the inner macula towards the foveola
(blocked fluorescence caused by yellow macular pig-
ments). FAF may be normal even in the presence of soft
or hard drusen.
Minimal change pattern
characterized by a limited and
irregular decrease or increase of background AF, not asso
ciated to any obvious or important topographic pattern.


