96
other fluorophores, extracellular fluid or degraded
photoreceptor remnants should be considered
(16)
(Fig. 18).
3.2.2.4 RPE tears
RPE tears usually occur in association with pigment epi
thelial detachments (PED) in patients with neovascular
AMD, either spontaneously or following therapy
(51)
.
FAF imaging reveals absence of autofluorescence in the
area denuded from RPE. These areas are clearly identifi-
able by their very low signal, whereas a heterogeneous
FAF signal is seen in the area where the RPE is rolled.
Therefore, the exact location of the tear can be delin-
eated in most cases. FAF imaging is a very good tool to
diagnose RPE tears
(34)
.
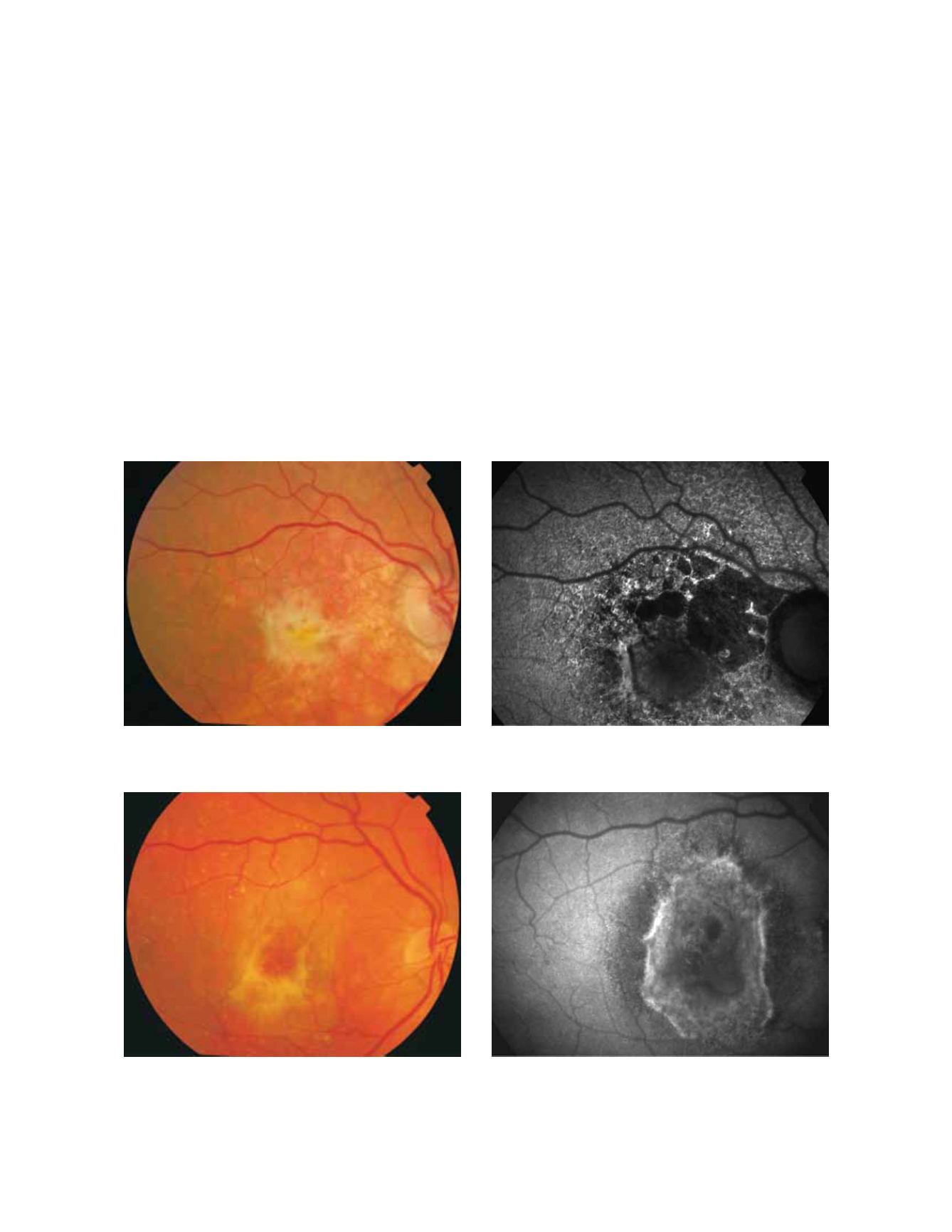
3.2.2.5 Disciform scars
The appearance of disciform scars in FAF imaging
depends on their duration and evolution
(34,36)
. Disciform
scars may show different variations and alterations
of FAF signal. A decreased signal is typically observed
in scarred and fibrotic areas. It has been reported that
approximately 50% of the disciform scars may be sur
rounded by a rim of increased FAF
(34,36)
. These areas
of increased autofluorescence correspond to irregularly
pigmented areas and may have been caused by a multi
layered RPE, a well illustrated finding in histopathology
(Fig. 19 and 20)
(35)
.
Figure 19 - Choroidal neovascularization with fibrosis. FAF outlines the marked atrophic lesions in the RPE surrounding the CNV /fibrosis. These
changes are inconspicuous in colour photographs. (A) Colour fundus and (B) fundus autofluorescence photographs.
Figure 20 - Fibrous scar secondary to CNV after treatment with anti-VEGF. The damaged RPE appears hyperpigmented in fundus photograph,
whereas FAF imaging shows an increased signal. (A) Colour fundus and (B) fundus autofluorescence photographs.
A
B
A
B


